Use the labels in the right column to find what you want. Or you can go thru them one by one, there are only 27,818 posts. Searching is done in the search box in upper left corner. I blog on anything to do with stroke.DO NOT DO ANYTHING SUGGESTED HERE AS I AM NOT MEDICALLY TRAINED, YOUR DOCTOR IS, LISTEN TO THEM. BUT I BET THEY DON'T KNOW HOW TO GET YOU 100% RECOVERED. I DON'T EITHER, BUT HAVE PLENTY OF QUESTIONS FOR YOUR DOCTOR TO ANSWER.
Changing stroke rehab and research worldwide now.Time is Brain!trillions and trillions of neuronsthatDIEeach day because there areNOeffective hyperacute therapies besides tPA(only 12% effective). I have 523 posts on hyperacute therapy, enough for researchers to spend decades proving them out. These are my personal ideas and blog on stroke rehabilitation and stroke research. Do not attempt any of these without checking with your medical provider. Unless you join me in agitating, when you need these therapies they won't be there.
What this blog is for:
My blog is not to help survivors recover, it is to have the 10 million yearly stroke survivors light fires underneath their doctors, stroke hospitals and stroke researchers to get stroke solved. 100% recovery. The stroke medical world is completely failing at that goal, they don't even have it as a goal. Shortly after getting out of the hospital and getting NO information on the process or protocols of stroke rehabilitation and recovery I started searching on the internet and found that no other survivor received useful information. This is an attempt to cover all stroke rehabilitation information that should be readily available to survivors so they can talk with informed knowledge to their medical staff. It lays out what needs to be done to get stroke survivors closer to 100% recovery. It's quite disgusting that this information is not available from every stroke association and doctors group.
Wednesday, February 7, 2018
fNIRS-based Neurorobotic Interface for gait rehabilitation
In this paper, a novel functional near-infrared spectroscopy (fNIRS)-based brain-computer interface (BCI) framework for control of prosthetic legs and rehabilitation of patients suffering from locomotive disorders is presented.
Methods
fNIRS signals are used to initiate and stop the gait cycle, while a nonlinear proportional derivative computed torque controller (PD-CTC) with gravity compensation is used to control the torques of hip and knee joints for minimization of position error. In the present study, the brain signals of walking intention and rest tasks were acquired from the left hemisphere’s primary motor cortex for nine subjects. Thereafter, for removal of motion artifacts and physiological noises, the performances of six different filters (i.e. Kalman, Wiener, Gaussian, hemodynamic response filter (hrf), Band-pass, finite impulse response) were evaluated. Then, six different features were extracted from oxygenated hemoglobin signals, and their different combinations were used for classification. Also, the classification performances of five different classifiers (i.e. k-Nearest Neighbour, quadratic discriminant analysis, linear discriminant analysis (LDA), Naïve Bayes, support vector machine (SVM)) were tested.
Results
The classification accuracies obtained from SVM using the hrf were significantly higher (p < 0.01) than those of the other classifier/ filter combinations. Those accuracies were 77.5, 72.5, 68.3, 74.2, 73.3, 80.8, 65, 76.7, and 86.7% for the nine subjects, respectively.
Conclusion
The control commands generated using the classifiers initiated and stopped the gait cycle of the prosthetic leg, the knee and hip torques of which were controlled using the PD-CTC to minimize the position error. The proposed scheme can be effectively used for neurofeedback training and rehabilitation of lower-limb amputees and paralyzed patients.
Neurological disability due specifically to stroke or spinal cord injury can profoundly affect the social life of paralyzed patients [1–3]. The resultant gait impairment is a large contributor to ambulatory dysfunction [4]. In order to regain complete functional independence, physical rehabilitation remains the mainstay option, owing to the significant expense of health care and the redundancy of therapy sessions. Such devices are developed as alternatives to traditional, expensive and time-consuming exercises in busy daily life. In the past, similar training sessions on treadmills performed using robotic mechanisms have shown better functional outcomes [1, 2, 5–7]. However, these devices have limitations particular to given research and clinical settings. Therefore, wearable upper- and lower-limb robotic devices have been developed [7, 8], which are used to assist users by actuating joints to partial or complete movement using brain intentions, according to individual-patient needs.
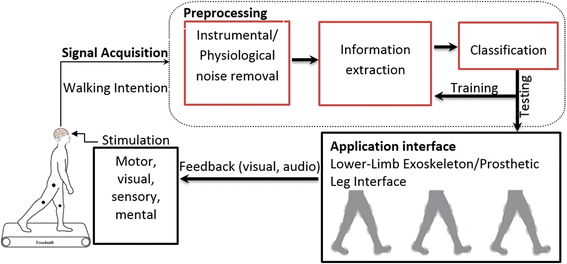
To date, various noninvasive modalities including functional magnetic resonance imaging (fMRI), electroencephalography (EEG) and functional near-infrared spectroscopy (fNIRS) have been used to acquire brain signals. fNIRS is a relatively new modality that detects brain intention with reference to changes in hemodynamic response. Its fewer artifacts, better spatial resolution and acceptable temporal resolution make it the choice for comprehensive and promising results in, for example, rehabilitation and mental task applications [9–20]. The main brain-computer interface (BCI) challenge in this regard is to extract useful information from raw brain signals for control-command generation [21–23]. Acquired signals are processed in the following four stages: preprocessing, feature extraction, classification, and command generation. In preprocessing, physiological and instrumental artifacts and noises are removed [24, 25]. After this filtration stage, feature extraction proceeds in order to gather useful information. Then, the extracted features are classified using different classifiers. Finally, the trained classifier is used to generate control commands based on a trained model [23]. Figure 1 shows a schematic of a BCI.
Fig. 1
Schematic of BCI
Previous studies on signal-acquisition techniques have shown promising outcomes, but rehabilitation applications require the best possible results [3, 4, 26]. In Eliana et al. [27], a treadmill was used to acquire EEG-based walking brain signals for sensorimotor applications with 87% accuracy. In Andreea et al. [28], EEG-based walking-intention signals were detected for stroke patients with an accuracy of 82%. Their data indicated that patients highly motivated for rehabilitation-related tasks tended to have higher success rates. In Naseer et al. [29], two-class motor imagery movements were analyzed using an LDA classifier. With their employed modality, fNIRS, the best features were found to be signal mean (SM) and signal slope (SS). By reducing the task period to between 2 and 7 s, the accuracies were improved to 77.56 and 87.28%, respectively. In Rea et al. [30], lower-limb movement for gait rehabilitation was detected based on fNIRS signals. They were able to acquire fNIRS signals in their chronic stroke patients during preparation for hip movement with 67.77 ± 11.35% accuracy. In Zhao et al. [31], a prosthetic controller was proposed for a bipedal robot. A walking gait pattern was found for the robot mechanism while an online optimized trans-femoral prosthesis control method (i.e. control Lyapunov function (CLF)-based quadratic programs (QPs) with variable impedance control) was tested on the knee and ankle joints of the prosthetic device. Azimi et al. [32] proposed stable robust adaptive impedance control for a prosthetic limb. A regressor-based nonlinear robust model was designed with reference to an adaptive impedance controller. In Richter et al. [33], dynamic modeling and simulation-based control of a prosthesis were performed, focusing on two-degree-of-freedom robot modeling, parametric estimation and feedback control for mimicking of hip motions. Perrey [34] explored neural gait control using fNIRS, specifically looking at the relevant cortical areas. In Venkatakrishnan [35], meanwhile, examined and discussed a rehabilitation-based brain machine interface (BMI) application for stoke patients.
The previous literature on the subject of rehabilitation shows that classification accuracy in the online setting is compromised by, among other problems, false triggering. Therefore, we also present a method to ensure that a correct command is always sent to a prosthetic leg (details are given in Section 3.1.1).
In this study, we acquired fNIRS walking signals of healthy subjects. Raw signals might contain noises and artifacts that can be removed using adaptive or band-pass filtering [25, 36]. In order to avoid such noises, the following six filters were compared for signal processing: Kalman, Wiener, finite impulse response (FIR), hemodynamic response (hrf), Band-pass, and Gaussian. Five classifiers, namely quadratic discriminant analysis (QDA), linear discriminant analysis (LDA), support vector machine (SVM), k-Nearest Neighbour (KNN), and Naïve Bayes (NB), were analyzed for acquisition of maximum classification accuracies. For offline BCI, SVM showed greater statistical significance (p < 0.01) as compared with the other classifiers; however, in consideration of execution delay and minimum computation cost, for online BCI, we used LDA with combinations of six features: SS, SM, signal peak (SP), signal kurtosis (KR), signal skewness (SK), and signal variance (SV). Walking intention was then used to initiate and stop the gait cycle of the proposed prosthetic leg model. For minimization of discomfort, a nonlinear computed torque controller (CTC) with gravity compensation was applied to two active joints in the hip and knee and one passive joint in the ankle for position control and reduction of error in waking patterns [37–39]. Given its effective simulation of classical limb-type and mobile robotics, the Peter Corke® robotics tool box was used to minimize position error [40]. The proposed system is applicable not only to paralyzed patients but also, and with little modification, to amputees and elderly people.

No comments:
Post a Comment